
MFA Interaction Design at Umeå Institute of Design
Duration: 8 weeks
Service design, Systems design, UX
Teamwork with Anuja Tripathi and Hao Zheng
Today’s healthcare system is based off of patients requesting help when a health issue arrises. Working with Nordic Rebels and VOPD (Vård och omsorg på distans — Healthcare and care with distance-spanning technologies) gave an invaluable insight on the existing initiatives to improve healthcare for people in low-density areas, common in the northern regions of Norway, Sweden and Finland. We would focus on the Swedish rural areas, studying them as a case study, to then expand upon and put into a grander scale.
Through their research, seminars, and the connections they had made through their own processes, a focus on treating people with existing issues in an unbalanced relationship with a healthcare provider became apparent. Throughout our study trip to Storuman the challenges were highlighted with living about 100 km from the nearest hospital and an aging population. To change the system radically, a solution would have to change the focus of the system.

Data could be aiding an early diagnosis, which will in its turn need complete sets of data. One big challenge with data collection is the security of it, ensuring a person’s integrity. By consolidating the data to the community and not only an individual, their privacy can be protected and secured. A functioning example of this method can be seen in academic research where data is gathered to reach conclusions, but is not connected to a person’s identity. Clear emphasis on providing consent to data sharing puts the inhabitant in charge of the moment and frequency of sharing the data or connecting the data to their person.
Empowering inhabitants (rather than patient) through frequent health monitoring is essential by giving them access to actionable data to prevent sickness. Acting early on small signs that your everyday well-being is deteriorating can greatly improve people’s health for longer. Small issues that become big problems can prevent the need to visit a healthcare provider and by making the gathered data actionable can motivate people to track and gather their data

When discussing the northern regions the negative is often highlighted; the challenges with providing services and systems to areas efficiently to fewer people, while the productive share of the population diminishes, ultimately leading to an aging population needing more services.
During our study trip we were able to talk to people there. Multiple had moved there for the high quality of life- when pressing on what this entails a common answer was the community.
Most inhabitants know or are acquainted with one another. This can prove to be an advantage when they need help. In healthcare the downside is that intimate information is hard to share with someone you know.
With few government run initiatives and specific needs connected to the area, the inhabitants of these remote municipalities have a can-do attitude engrained. They would fill in the gaps themselves and provide solutions when needed, helping each other out. This was the case when suicide rattled Storuman and the municipality contacted local researchers to help find out ways to prevent this from happening.
In a community based healthcare system the healthcare provider acts as a coach/guide and becomes part of the community, where mutual respect is shown and all parties take care of each other.

Connecting the healthcare provider and the inhabitant through communities and AI, the gathered data can be processed. The mundane data points are sorted out by AI, to highlight the points that could be improved and are actionable. The inhabitant can discuss these actionable points with the community, provided by empathy and support, while being mentored by the healthcare provider.
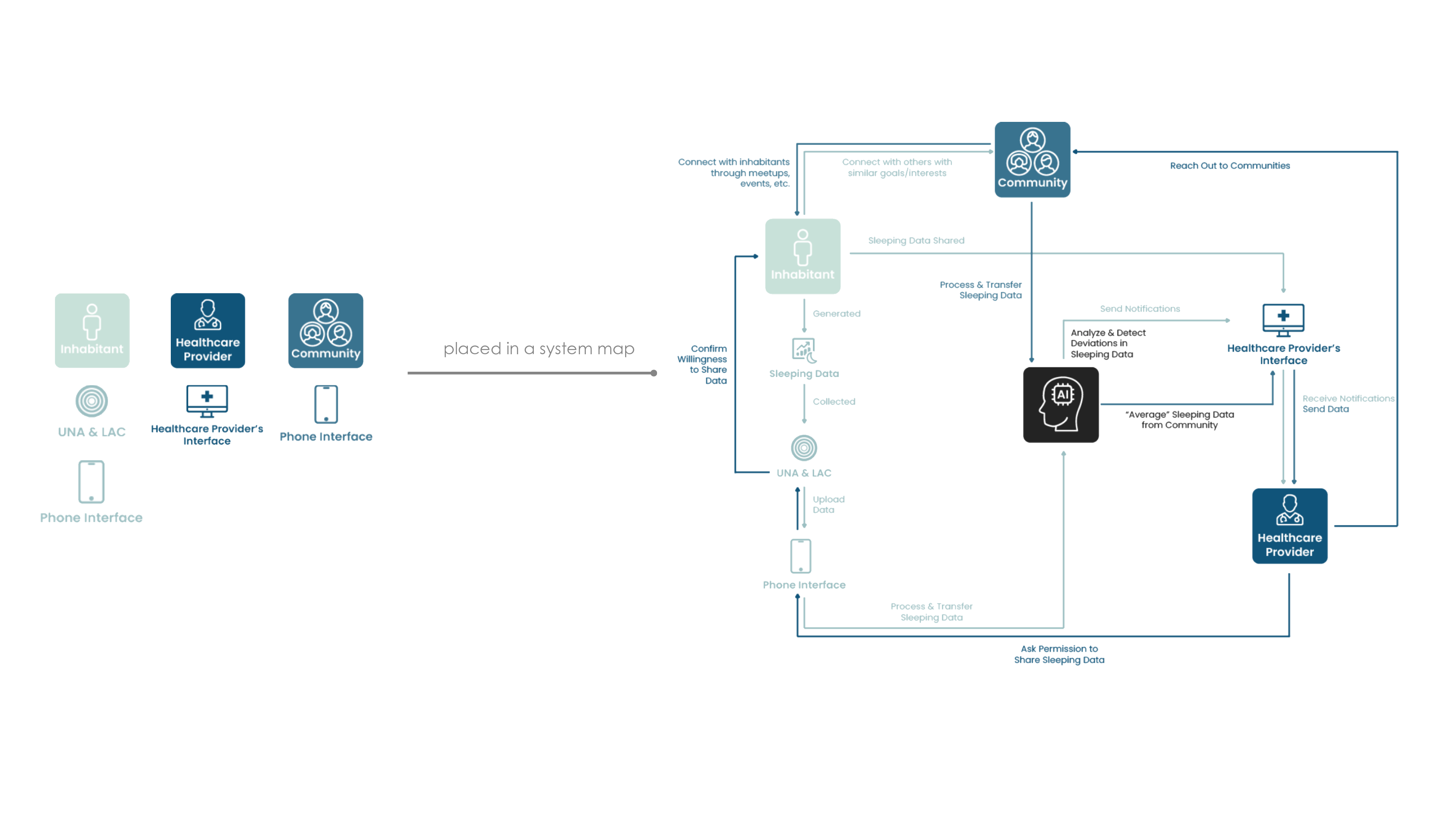
The touchpoints for each of these actors are connected to the needs that arise. The inhabitant has a combination of tangible artefacts and digital interface. The healthcare provider and the communities are tied to the digital interfaces.
The digital interface acts as a data lake (Lacuna meaning lake in Latin) with specific functions to engage and motivate. The tangible artefacts enhance the interaction by making certain actions more deliberate than what can be achieved through digital interfaces.
A challenge that is easily overlooked is how to maintain, and even, improve a humane and empathetic approach to healthcare in the future.
Una is the tangible part of the inhabitant’s data tracking. It acts both as:

By making the action of sharing the data physical, the inhabitant performs this on a more conscious level, making the action and choice to do so deliberate.
The healthcare provider has an overview of the people in the community they are mentoring. Notifications when data is deviating from the standard enables them to help people specifically when needed; to see what is happening in detail the healthcare provider requests access from the inhabitant.

The inhabitant can grant this request by using UNA and the interface. Only then will their data be connected with their identity.Otherwise the data is cumulated with the community’s data.
Inhabitants are prompted to join communities based on their data and their interests. These communities consist of others with similar issues, empowering them to provide and access empathy, support and new resources.

New connections and patterns can be uncovered by talking to others with a similar situation in ways that are hard for someone with an outside perspective.
Events, lectures, etc. engage the inhabitants in these communities, bringing in the healthcare provider as a mentor for the larger group of people.
When engaging in these communities, the inhabitant can set the level of anonymity, disclosing the information they are comfortable such as their name, geographical location and picture.
The healthcare provider connects with a larger group, setting up lectures, workshops or open Q&A’s- according to what is needed in the group.Through these interactions mutual learning can be established as an ongoing dialogue occurs; the inhabitants learn a great deal from each other and between healthcare providers.



For the healthcare provider
In the community view, the healthcare provider is notified of inhabitants with deviating data. They then request access to the inhabitant’s data. The inhabitant grants the access by placing their UNA on the interface.
Granted access to the inhabitant’s detailed data, the healthcare provider gets an initial recommendation generated by AI. This can alleviate the healthcare provider from having to interact with simple or basic counselling. The healthcare provider can also tweak the recommendation.
Once confirmed, the recommendation is sent to the inhabitant.

Throughout this project, the team performed minimal user testing. This was done consciously to focus on the systematic level of the challenge with distance spanning healthcare.
As there is an abundance of solutions available for specific diagnoses, the challenging aim was to look into a higher level abstraction (away from concrete solutions). When interacting with local researchers in northern Sweden, an analogy was made where these specific solutions could be seen as fruit, making a great fruit salad. But there is no recipe available for the fruit salad; what is the overarching design?
In the final moments of the project the solution was made into very concrete solutions, combining physical and digital interactions, to highlight the challenges when it comes to changing healthcare systems.
This makes this design not so much a solution — rather a proposal. A proposal which can be researched further. User testing should be done based on a gradual implementation: It should only be done gradually, as change is hard to accept.